
GLP-1 medications are often framed as a recent breakthrough.
But, for people living with diabetes, they’ve been part of the treatment landscape for years.
These medications were developed and studied first for glycemic control, not weight loss—and the science behind them continues to evolve.
I’m writing this as both a health coach and a person with diabetes who has personally taken a GLP-1.
That perspective matters.
Understanding how these medications work in real bodies is key to using them effectively and safely.
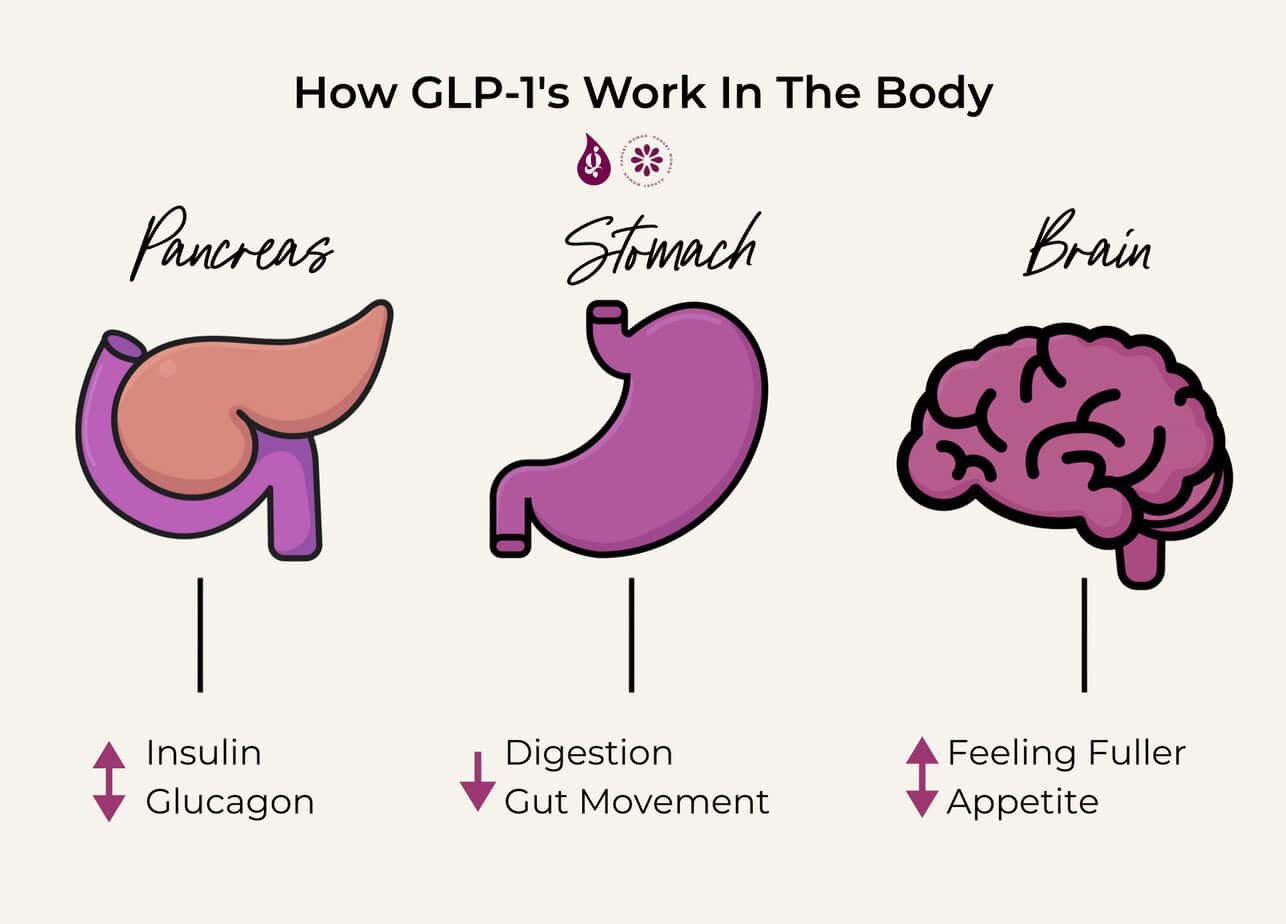
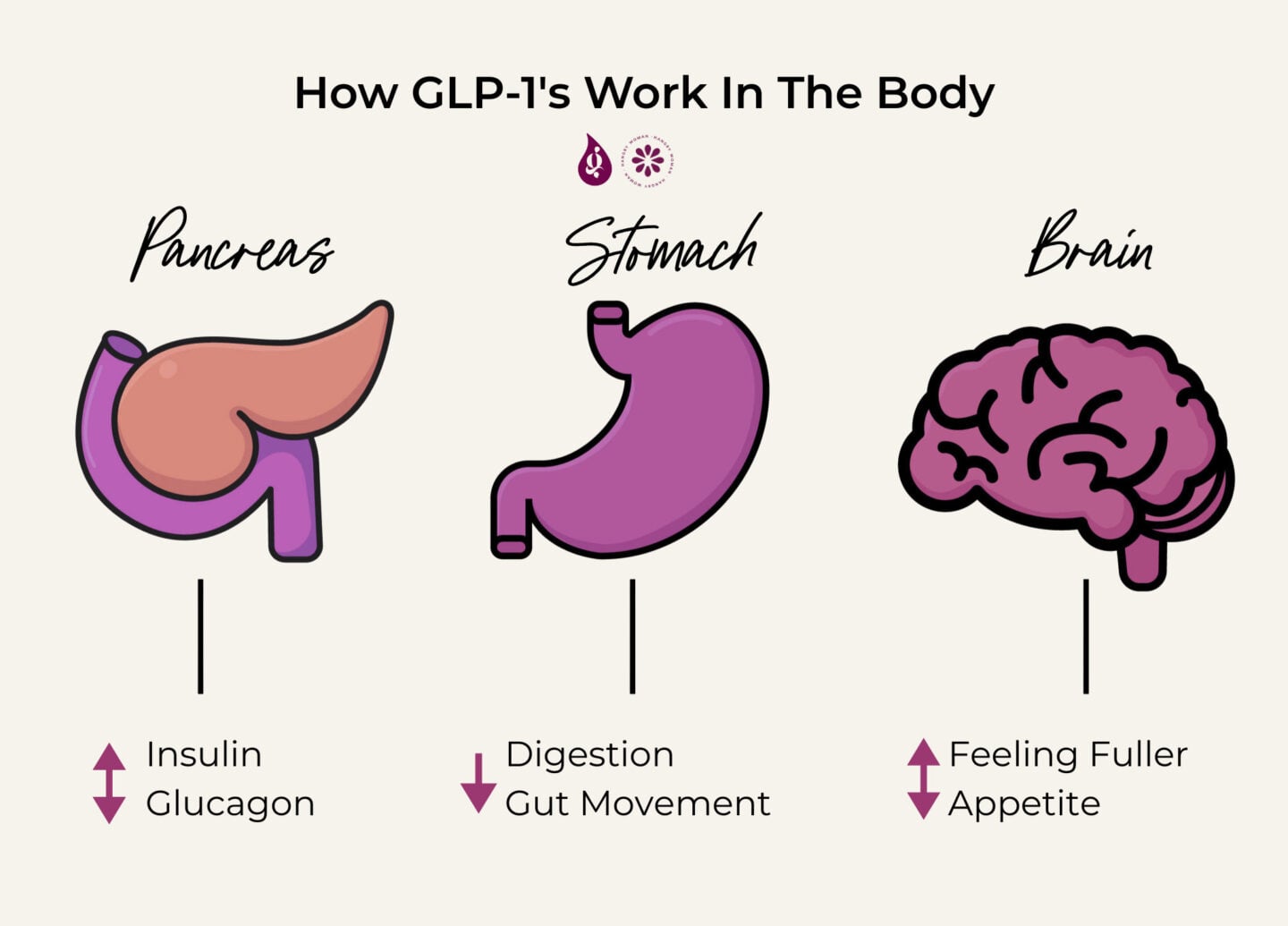
How GLP-1 Medications Work in the Body
GLP-1 stands for glucagon-like peptide-1, a naturally occurring gut hormone involved in blood sugar regulation. GLP-1 receptor agonists mimic and enhance this hormone’s effects.
Specifically, GLP-1 medications:
• Increase glucose-dependent insulin secretion¹
• Suppress glucagon release after meals¹
• Slow gastric emptying, reducing rapid post-meal glucose excursions²
• Influence appetite regulation through central nervous system pathways³
This is why GLP-1 medications improve glycemic control without directly forcing insulin release when blood sugar is already low.
Clinical studies consistently show improved after-meal blood sugar control and reduced overall glycemic variability in people with type 2 diabetes using GLP-1 receptor agonists¹².
Types of GLP-1 Medications Used in Diabetes Care
Brand Names of GLP-1 Medications
Several GLP-1 receptor agonists are FDA-approved for diabetes management, and each is marketed under specific brand names.
Semaglutide is sold under the brand names Ozempic (a once-weekly injectable for type 2 diabetes) WeGovy, an injectable for weight loss and Rybelsus (the oral formulation taken daily).
Dulaglutide is marketed as Trulicity, a once-weekly injectable GLP-1 receptor agonist.
Liraglutide is available as Victoza, which is administered daily for diabetes management.
Tirzepatide, while technically a dual GIP/GLP-1 receptor agonist rather than a GLP-1-only medication, is prescribed under the brand name Mounjaro for type 2 diabetes and is often discussed alongside GLP-1 therapies because of its similar—and in some cases amplified—mechanisms of action.
These medications are administered via subcutaneous injection, typically once weekly (daily for some formulations).
Large randomized controlled trials have demonstrated that these injectable agents significantly lower HbA1c and improve cardiometabolic markers compared to placebo or other glucose-lowering therapies⁴⁵.
Oral GLP-1 Medication
Oral semaglutide is currently the only oral GLP-1 receptor agonist available. While effective, its absorption is sensitive to timing, fasting state, and gastric conditions, which may limit feasibility for some individuals⁶.
Benefits of GLP-1 Medications for Diabetes Management
Reduction in HbA1c
Across multiple large trials, GLP-1 receptor agonists have been shown to reduce HbA1c by approximately 1–1.5 percentage points, depending on dose and individual response⁴⁵⁷.
This reduction reflects improved long-term glycemic exposure rather than isolated improvements in daily readings.
Appetite Regulation and Weight Effects
GLP-1 medications also influence appetite regulation by increasing signals to your brain that you’re feeling full, or satiety³. Many individuals report reduced hunger, earlier fullness, and decreased food-related preoccupation, or food noise.
Weight loss is a secondary physiological effect, not the primary goal in diabetes treatment, though it has been consistently observed in clinical trials⁵⁶.
Side Effects and Safety Considerations
Common Side Effects
The most frequently reported side effects—particularly during dose escalation—include nausea, early satiety, constipation, and diarrhea. These effects are dose-dependent and often go away the longer you use the medication⁶⁷.
Increasing the dose slowly, and over time can make an impact on side effects⁷.
Serious Risks of GLP-1 Receptor Agonists.
GLP-1 receptor agonists are not recommended in individuals with a personal or family history of medullary thyroid carcinoma or MEN2 syndrome⁶.
Patients with severe gastroparesis may also experience discomfort due to delayed gastric emptying effects.
For individuals using insulin or insulin secretagogues, dose adjustments may be required to reduce hypoglycemia risk⁸.
Cost and Accessibility of GLP-1 Medications
While GLP-1 receptor agonists are clinically effective, they are also among the most expensive diabetes medications on the market, and access varies widely depending on insurance coverage, indication, and geography.
For people with type 2 diabetes, medications like Ozempic, Trulicity, Victoza, and Mounjaro are more likely to be covered by insurance—but coverage is rarely automatic.
Prior authorizations are common, and insurers often require documentation showing that other medications were tried first. Even with coverage, copays can range from manageable to eye-watering, depending on the plan.
Without insurance, monthly list prices for GLP-1 medications can exceed $900–$1,300, putting them out of reach for many people.
Manufacturer savings cards may reduce costs for some patients with commercial insurance, but these programs often exclude people on Medicare, Medicaid, or other public insurance plans—ironically the populations with the highest rates of diabetes.
Access challenges also show up in supply availability. In recent years, increased demand—particularly for weight-loss indications—has led to shortages, delayed refills, and forced medication switches.
For people managing diabetes, these disruptions aren’t just inconvenient; they can directly affect blood sugar stability and treatment.
From a health equity standpoint, this creates a real problem: medications with strong evidence for improving glycemic and cardiovascular outcomes are not equally accessible, and cost can become a barrier that shapes care more than clinical need.
This is why GLP-1s are best discussed not as a universal solution, but as one option within an individualized diabetes plan—one that accounts for affordability, insurance realities, and long-term sustainability.
In practice, many people end up making decisions not based on what works best for their bodies, but on what they can consistently access.
Using GLP-1 Medications Effectively
Clinical guidelines emphasize individualized dosing, gradual escalation, and regular glucose monitoring to assess medication response⁸.
From a coaching perspective, effective use also includes:
• Monitoring trends rather than isolated readings
• Adjusting concurrent therapies thoughtfully
• Paying attention to digestion, energy, and hunger signals
Medication works best when paired with education and context.
What Recent Research Shows
Over the past decade, GLP-1 receptor agonists have shown:
• Reduced cardiovascular risk in people with type 2 diabetes⁴⁵
• Improved kidney outcomes in high-risk populations⁹
• Sustained glycemic improvements with long-term use⁸
Ongoing trials continue to evaluate combination therapies, long-term safety, and broader metabolic benefits.
How Glucose Guide Supports People Using GLP-1 Medications
GLP-1 medications provide biological support—but they don’t teach you how your body responds to food, timing, or lifestyle changes. That’s where Glucose Guide fills the gap.
Step 1: Joining Glucose Guide
When you join Glucose Guide, you gain access to a structured diabetes support system built around real-world decision-making, not perfectionism.
Step 2: Track With Context
The Diabetes Food Journal allows you to log meals, blood sugars, medications, and symptoms together—creating a full picture rather than isolated data points.
Step 3: Identify Meaningful Patterns
Over time, Glucose Guide helps you see how GLP-1 dosing, food choices, and timing interact with blood sugar trends. This insight supports safer adjustments and more productive medical conversations.
Step 4: Build Sustainable Confidence
Glucose Guide combines education, community support, and coaching-informed tools to help people with diabetes:
• Reduce guesswork
• Improve self-advocacy
• Build habits that align with medication therapy
GLP-1s are not a replacement for education or lived experience. Glucose Guide helps integrate all of it into a system that supports long-term health goals.
Talk to your doctor about the process, pros and cons for your individual goals if you’re interested in beginning a GLP-1
References
- Holst J. J. (2007). The physiology of glucagon-like peptide 1. Physiological reviews, 87(4), 1409–1439. https://doi.org/10.1152/physrev.00034.2006
- Wölnerhanssen, B. K., Meyer-Gerspach, A. C., Peters, T., Beglinger, C., & Peterli, R. (2016). Incretin effects, gastric emptying and insulin responses to low oral glucose loads in patients after gastric bypass and lean and obese controls. Surgery for obesity and related diseases : official journal of the American Society for Bariatric Surgery, 12(7), 1320–1327. https://doi.org/10.1016/j.soard.2015.11.022
- Farr, O. M., Sofopoulos, M., Tsoukas, M. A., Dincer, F., Thakkar, B., Sahin-Efe, A., Filippaios, A., Bowers, J., Srnka, A., Gavrieli, A., Ko, B. J., Liakou, C., Kanyuch, N., Tseleni-Balafouta, S., & Mantzoros, C. S. (2016). GLP-1 receptors exist in the parietal cortex, hypothalamus and medulla of human brains and the GLP-1 analogue liraglutide alters brain activity related to highly desirable food cues in individuals with diabetes: a crossover, randomised, placebo-controlled trial. Diabetologia, 59(5), 954–965. https://doi.org/10.1007/s00125-016-3874-y
- Marso, S. P., Daniels, G. H., Brown-Frandsen, K., Kristensen, P., Mann, J. F. E., Nauck, M. A., Nissen, S. E., Pocock, S., Poulter, N. R., Ravn, L. S., Steinberg, W. M., Stockner, M., Zinman, B., Bergenstal, R. M., & Buse, J. B. (2016). Liraglutide and cardiovascular outcomes in type 2 diabetes. New England Journal of Medicine, 375(4), 311–322. https://doi.org/10.1056/NEJMoa1603827
- Gerstein, H. C., Colhoun, H. M., Dagenais, G. R., Diaz, R., Lakshmanan, M., Pais, P., Probstfield, J., Riesmeyer, J. S., Riddle, M. C., Rydén, L., Xavier, D., Atisso, C. M., Dyal, L., Hall, S., Rao-Melacini, P., Wong, G., Avezum, A., Basile, J., Chung, N., Conget, I., … REWIND Investigators (2019). Dulaglutide and cardiovascular outcomes in type 2 diabetes (REWIND): a double-blind, randomised placebo-controlled trial. Lancet (London, England), 394(10193), 121–130. https://doi.org/10.1016/S0140-6736(19)31149-3
- Davies, M., Pieber, T. R., Hartoft-Nielsen, M. L., Hansen, O. K. H., Jabbour, S., & Rosenstock, J. (2017). Effect of Oral Semaglutide Compared With Placebo and Subcutaneous Semaglutide on Glycemic Control in Patients With Type 2 Diabetes: A Randomized Clinical Trial. JAMA, 318(15), 1460–1470. https://doi.org/10.1001/jama.2017.14752
- Here is the APA 7th edition citation, formatted to publication standards:
- Frias, J. P., Davies, M. J., Rosenstock, J., Pérez Manghi, F. C., Fernández Landó, L., Bergman, B. K., Liu, B., Cui, X., Brown, K., & SURPASS-2 Investigators. (2021). Tirzepatide versus semaglutide once weekly in patients with type 2 diabetes. New England Journal of Medicine, 385(6), 503–515. https://doi.org/10.1056/NEJMoa2107519
- American Diabetes Association Professional Practice Committee. (2024). 9. Pharmacologic approaches to glycemic treatment: Standards of care in diabetes—2024. Diabetes Care, 47(Supplement 1), S158–S178. https://doi.org/10.2337/dc24-S009
- Granata, A., Maccarrone, R., Anzaldi, M., Leonardi, G., Pesce, F., Amico, F., Gesualdo, L., & Corrao, S. (2022). GLP-1 receptor agonists and renal outcomes in patients with diabetes mellitus type 2 and diabetic kidney disease: state of the art. Clinical kidney journal, 15(9), 1657–1665. https://doi.org/10.1093/ckj/sfac069